


Transitioning an AAV gene therapy program from adherent cell culture to a suspension platform is one of the highest-stakes CMC decisions a sponsor will make. Done well, it unlocks the scale, cost, and process control needed for late-phase and commercial supply. Done poorly, it introduces comparability gaps that can stall an IND amendment or, worse, force a return to the original platform after months of work.
This guide walks through the technical, analytical, and regulatory considerations for making the transition safely — written for CMC, process development, and manufacturing leaders who are actively scoping or executing this work.
Why teams transition from adherent to suspension
Adherent platforms — most commonly HEK293 cells grown on cell stacks, roller bottles, or fixed-bed bioreactors like the iCELLis — have historically dominated early-stage AAV production. They produce high-quality vector and are well-understood by process scientists. But they hit a hard ceiling.
The economics and operational case for suspension typically becomes compelling around the Phase 2 transition or earlier for systemic indications. Specifically:
- Linear scalability. Suspension processes scale by volume in stirred-tank bioreactors (50L → 200L → 2,000L). Adherent processes scale by surface area, which means more units, not bigger units — a labor and footprint nightmare at commercial scale.
- Cost of goods. A 2,000L suspension run can produce vector quantities that would require dozens of iCELLis 500 runs to match, with a fraction of the consumables and labor.
- Process control. Stirred-tank bioreactors offer superior real-time monitoring of pH, DO, temperature, and metabolites — critical for process characterization and PPQ.
- Closed-system manufacturing. Suspension processes are more readily closed end-to-end, supporting better contamination control and aligning with FDA’s expectations around advanced manufacturing.
That said, the transition is non-trivial. The cell line behaves differently, transfection chemistry must be re-optimized, and analytical comparability is the gating regulatory question.
Pre-transition readiness checklist of 5 questions to ask:
Before committing resources, run an honest internal assessment:
- Is the adherent process locked, with a stable reference standard and well-characterized critical quality attributes (CQAs)?
- Do you have analytical methods that are platform-agnostic (i.e., they measure the vector, not the process)?
- Are CQA acceptance ranges defined with enough data to support a comparability assessment?
- Do you have regulatory alignment — ideally a Type B or Type C meeting where transition strategy was discussed?
- Is there budget and timeline tolerance for a 12-18 month effort with realistic failure modes built in?
If you answered no to two or more, slow down. Premature transitions typically fail not at the bioreactor but at the comparability stage, when regulators see drift in capsid content, aggregation, or potency that cannot be unambiguously linked to platform versus process versus analytical noise.
Cell line and media selection
The first technical decision is the suspension-adapted host cell line. The dominant options in AAV production today are:
- HEK293 suspension variants — Expi293F (Thermo Fisher), Viral Production Cells (VPC 2.0), and proprietary suspension-adapted HEK293 lines developed internally or by CDMOs. These are the most common choice because the regulatory and analytical bridge from adherent HEK293 is shorter.
- Sf9 / baculovirus systems — A fundamentally different platform that some sponsors consider in parallel. We won’t cover that path here; it’s not a transition, it’s a switch.
For HEK293 suspension transitions, the most common path is to source a vendor-qualified suspension line with a clear regulatory history (master cell bank documentation, viral safety testing, identity confirmation by STR profiling). Using a line with a documented provenance dramatically simplifies the FDA’s CMC review of your cell substrate.
Media selection is equally consequential. Chemically defined, animal-component-free media (BalanCD HEK293, FreeStyle F17, Expi293 Expression Medium) are the standard. Two pitfalls to avoid:
- Don’t lock in a single-source proprietary medium without negotiating long-term supply agreements. Several AAV programs have been forced into media re-qualification mid-clinical because the formulation changed or supply faltered.
- Don’t underestimate the feed strategy. Suspension AAV production at high cell density is metabolically demanding; lactate accumulation and ammonia toxicity can crater specific productivity if feed is not optimized.
Transfection optimization in suspension
This is where most transitions stumble. Triple-transfection with PEI (polyethylenimine) remains the dominant approach for AAV in suspension, but the optimal parameters in suspension differ meaningfully from adherent.
Key variables to optimize, ideally in a DoE framework:
- Cell density at transfection (TCD). Typically 1.5-4 × 10⁶ cells/mL. Too low and yield per liter suffers; too high and the “density effect” suppresses per-cell productivity.
- PEI:DNA ratio. Usually 2:1 to 4:1 (w/w). Higher ratios increase transfection efficiency but also cytotoxicity.
- Total DNA per million cells. 1-2 µg per 10⁶ cells is a common starting range.
- Plasmid ratio (Rep/Cap : helper : transgene). Often 1:1:1 by mass, but molar ratio optimization can improve full:empty ratios.
- Plasmid quality. Endotoxin, supercoiled percentage, and homogeneity matter more in suspension than adherent. GMP-grade plasmid is typically required by the IND-enabling tox lot.
- Harvest timing. 48-96 hours post-transfection, depending on serotype and process.
A well-run optimization in shake flasks and small bioreactors (Ambr 250 is the workhorse here) will burn 4-8 months. Compress this at your peril — sloppy transfection optimization is the most common root cause of low titer and high empty capsid percentages downstream.
Illustrative process yield comparison
The figure below shows a representative comparison of total vector genome yield across platforms at equivalent batch sizes. Numbers are illustrative and vary widely by serotype, transgene, and process maturity.
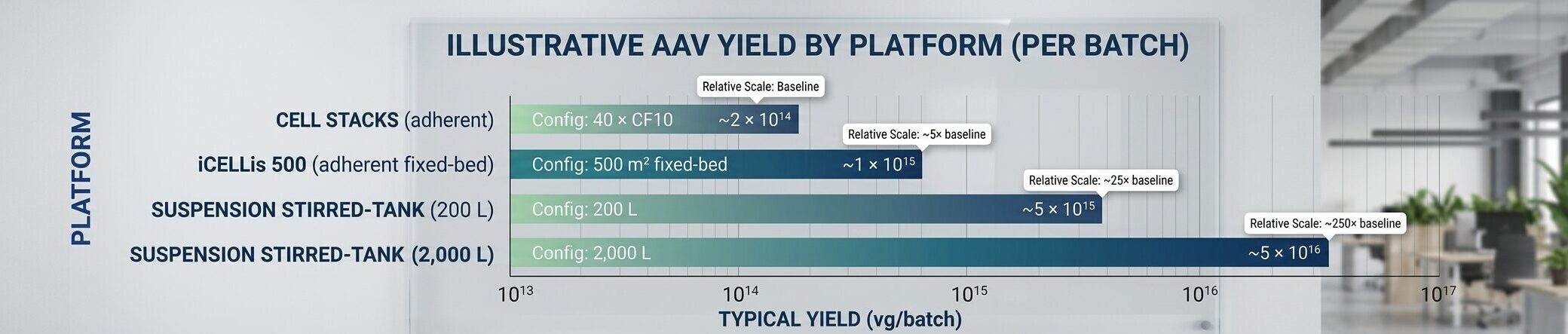
| Platform | Configuration | Typical Yield (vg/batch) | Relative Scale |
|---|---|---|---|
| Cell Stacks (adherent) | 40 × CF10 | ~2 × 10¹⁴ | Baseline |
| iCELLis 500 (adherent fixed-bed) | 500 m² fixed-bed | ~1 × 10¹⁵ | ~5× baseline |
| Suspension stirred-tank | 200 L | ~5 × 10¹⁵ | ~25× baseline |
| Suspension stirred-tank | 2,000 L | ~5 × 10¹⁶ | ~250× baseline |
Order-of-magnitude comparison; actual yields vary significantly by serotype, transgene, transfection optimization, and process maturity.
The takeaway is not that suspension is universally “better” — it’s that the productivity and scalability ceiling is dramatically higher, which is why the transition is worth the regulatory and analytical investment for any program targeting late-stage trials or commercial supply.
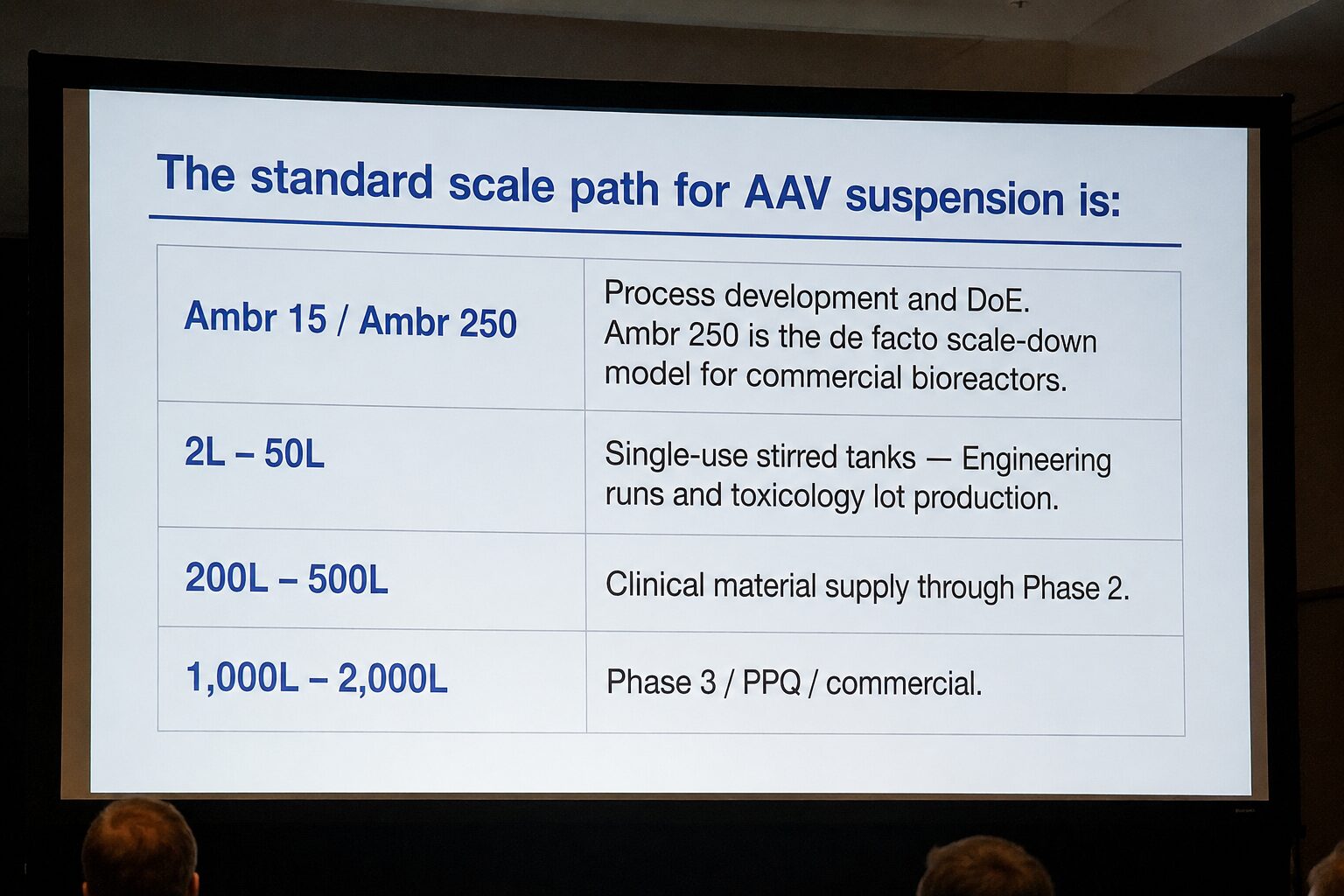
Bioreactor selection and scale-down models
The standard scale path for AAV suspension is:
- Ambr 15 / Ambr 250 — Process development and DoE. Ambr 250 is the de facto scale-down model for commercial bioreactors.
- 2L – 50L single-use stirred tanks — Engineering runs and toxicology lot production.
- 200L – 500L — Clinical material supply through Phase 2.
- 1,000L – 2,000L — Phase 3 / PPQ / commercial.
Single-use bioreactor systems from Cytiva (Xcellerex), Thermo Fisher (HyPerforma), Sartorius (Biostat STR), and others dominate this space. The choice between platforms is driven by your CDMO relationships, geometric scalability, and your willingness to commit to a vendor ecosystem for sensors, bags, and consumables.
Critically, your scale-down model must be qualified — meaning you demonstrate that the small-scale system predicts large-scale performance for your CQAs. This is non-negotiable for process characterization and PPQ readiness.
Analytics and comparability
Comparability is the regulatory linchpin of the entire transition. The FDA’s 2020 guidance on CMC information for human gene therapy INDs sets the expectation: any change to the manufacturing platform requires a comparability assessment demonstrating that the post-change product is comparable to pre-change in identity, purity, potency, and safety.
For an adherent-to-suspension transition, expect to provide head-to-head data on:
- Identity — capsid serotype confirmation, transgene sequence integrity
- Vector genome titer — typically ddPCR or qPCR, with orthogonal method confirmation
- Capsid titer and full:empty ratio — analytical ultracentrifugation (AUC), charge-detection mass spectrometry (CDMS), or cryo-EM
- Potency — cell-based functional assays appropriate to the transgene’s mechanism
- Purity — residual host cell protein, host cell DNA, plasmid DNA, BSA
- Aggregation and particle characterization — DLS, SEC-MALS
- Post-translational modifications and capsid PTMs — increasingly expected by regulators
Robust analytical method development is the foundation of comparability. If your methods drift or have high variability, you cannot distinguish platform effects from analytical noise — and reviewers will hold this against you. Methods should be qualified before the transition begins, not retrofitted after the fact.
Beyond analytics, the broader quality control infrastructure — reference standards, retain samples, stability programs — must be aligned across both platforms during the bridging period.
Regulatory strategy and timing
Engage FDA early. A Type B meeting (for an active IND) or Type C meeting (for general guidance) to align on comparability strategy is one of the highest-value activities in the entire transition. Specific topics worth raising:
- Acceptance criteria for comparability — what’s the agency’s expectation for analytical match versus statistical equivalence?
- Whether bridging toxicology will be required (often no for AAV if comparability is robust, but ask)
- Timing of the platform change relative to pivotal trials — agencies strongly prefer the change to occur before pivotal, not during
- Stability bridging — how much stability data on the suspension-produced material is needed at the time of the change?
Document everything. Maintain a side-by-side process comparability matrix that tracks every CPP (critical process parameter) and CQA across both platforms. This becomes the backbone of your CMC amendment and your eventual BLA.
5 Common failure modes
The transitions that fail tend to fail in predictable ways:
- Underestimating transfection optimization. Teams assume adherent transfection conditions translate. They don’t.
- Low full:empty ratios. Suspension processes can produce higher empty capsid percentages without careful optimization, complicating downstream purification and dose specification.
- Inadequate scale-down qualification. The Ambr 250 looked great; the 200L doesn’t reproduce it.
- Analytical drift during the transition. Method revisions during the bridging period make comparability uninterpretable.
- Regulatory ambiguity. Sponsors who don’t engage the FDA on comparability strategy often discover misalignment only at the CMC amendment review — a costly time to find out.
Realistic 1.5 year timeline and cost
For a program with an established adherent process and competent CMC organization, plan for 12-18 months from kickoff to first suspension GMP lot. A representative timeline:
- Months 1-3: Cell line, media, and transfection screening (shake flask)
- Months 3-6: DoE optimization in Ambr 250
- Months 6-9: Scale-up to 50L engineering runs
- Months 9-12: GMP engineering and toxicology lot production
- Months 12-15: Comparability studies and analytical bridging
- Months 15-18: CMC amendment preparation and submission
Direct costs typically run $3-7M for the technical work alone, excluding GMP slot fees at a CDMO. Including CDMO engineering and GMP runs, total cost of $8-15M is realistic for a program executing this externally.
5 Common Questions We Often Hear:
Do we need to repeat IND-enabling toxicology after the transition?
-
- Usually no, if comparability is robust and the product profile is unchanged. The FDA’s position is risk-based: if the suspension-produced material is analytically and functionally comparable to the adherent material that supported the original tox package, bridging toxicology is typically not required. That said, the agency reserves the right to ask, and the bar for “robust” is higher than many sponsors initially assume.
Can we run adherent and suspension in parallel during clinical trials?
-
- Yes, and many programs do — typically using adherent material for ongoing patients and suspension for new enrollment after comparability is established. This requires careful lot tracking and pharmacovigilance, and the FDA will want to see both materials represented in safety analyses.
How do we handle reference standard during the transition?
-
- Maintain the existing adherent-produced reference standard through the transition, and qualify a new suspension-produced reference standard against it. This bridges your historical data and your future data. Eventually the suspension reference becomes primary, but the bridging period is critical.
Is the empty:full ratio inherently worse in suspension?
-
- Not inherently — but suspension processes tend to be less forgiving of suboptimal transfection conditions, so unoptimized suspension processes often show higher empty percentages than mature adherent processes. With proper DoE optimization, suspension processes can match or exceed adherent on full:empty ratios.
What’s the most underappreciated risk in this transition?
-
- Analytical method robustness. Sponsors invest enormous effort in the process and underinvest in the assays that measure it. When comparability data is noisy, you cannot tell whether the platform changed the product or your assay drifted. Method qualification before the transition starts is the single highest-leverage investment.
The TLDR on Transitioning an AAV Gene Therapy Program in 2026
The adherent-to-suspension transition is a defining CMC milestone for any AAV program targeting late-phase or commercial supply. It is technically demanding, regulatorily consequential, and unforgiving of shortcuts — but the programs that execute it well unlock the manufacturing economics required to deliver gene therapy at scale.
DES Pharma Consulting supports gene therapy sponsors through platform transitions, comparability strategy, and FDA engagement. If your program is approaching this inflection point, the time to plan is now — not when the IND amendment is due.

Meade has 15 years of dedicated experience in the biopharmaceutical industry, specializing in bioprocess design, scale-up, manufacturing, and IND-enabling CMC strategy across advanced therapy and biologics programs.
Reach out to Meade on LinkedIn.


