


A pre-IND meeting is one of the highest-leverage interactions a biologics sponsor will have with FDA before clinical trials begin. Used well, it surfaces and resolves regulatory questions before they become IND clinical hold issues. Used poorly — with a thin briefing package or vague questions — it produces non-committal agency responses that leave you exactly where you started.
The CMC section of the briefing package is where most sponsors either build agency confidence or signal that they’re not yet ready. This guide walks through what FDA expects to see in the CMC content for a novel biologic, how to scope it appropriately given typical pre-IND stage maturity, and how to use the meeting to de-risk your IND submission.
What a pre-IND meeting actually is
A pre-IND meeting is a Type B meeting under FDA’s formal meeting framework, requested by the sponsor before the IND is submitted. The agency uses these meetings to provide guidance on the adequacy of the development program — clinical, nonclinical, and CMC — to support an IND.
Pre-IND meetings are not approvals. FDA will not “approve” your CMC plan or commit to accepting your IND. What you get is alignment on agency expectations, identification of gaps, and an opportunity to surface specific questions that, if you wait until IND review to ask, will appear as deficiencies in a clinical hold letter.
For novel biologics — meaning products that are first-in-class, use novel modalities, novel manufacturing platforms, or novel routes of administration — pre-IND engagement is especially valuable. The novelty is exactly what creates regulatory uncertainty, and FDA prefers to identify that uncertainty before reading your IND.
How CMC content fits into the briefing package
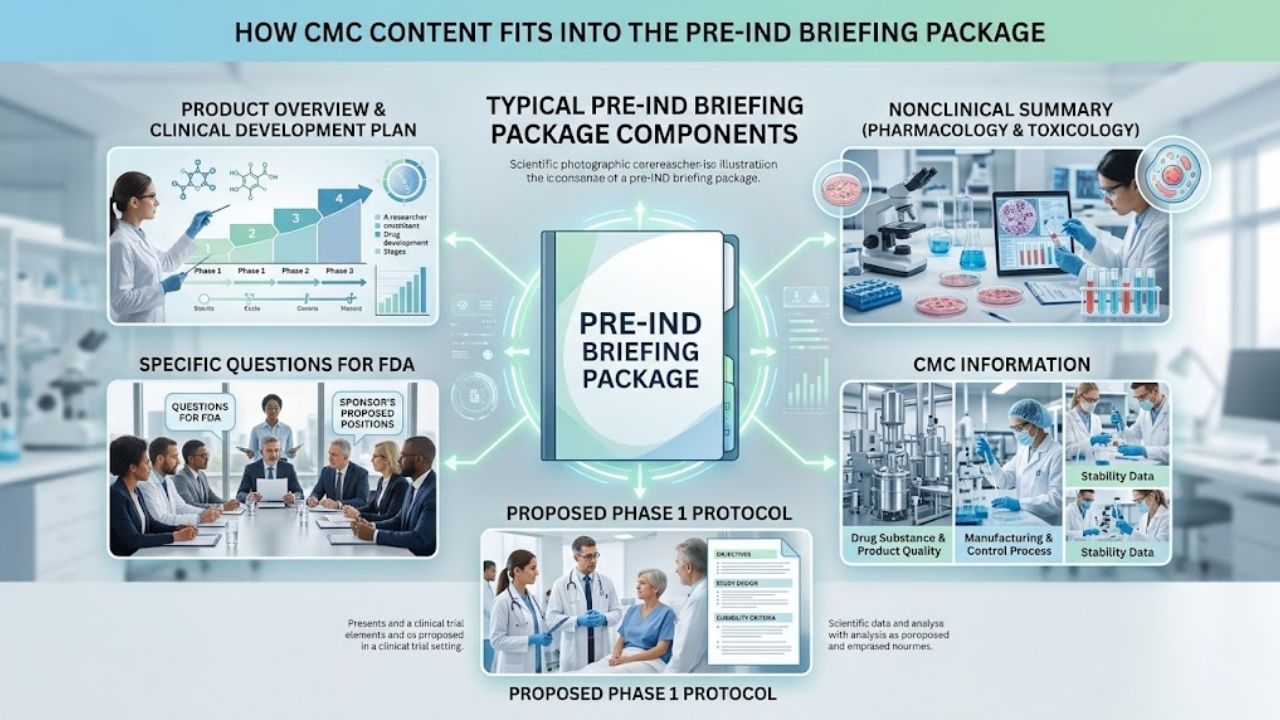
A pre-IND briefing package typically includes:
- Product overview and clinical development plan
- Nonclinical (pharmacology and toxicology) summary
- CMC information
- Proposed Phase 1 protocol synopsis or full protocol
- Specific questions for FDA, with sponsor’s proposed positions
The CMC section’s purpose is to give FDA enough information to assess whether the manufacturing, characterization, and control strategy is appropriate to support the proposed Phase 1 trial. It is not the IND CMC module. It is not a full CTD-format submission. It is a focused summary that supports the specific questions you’re asking.
What FDA expects to see in the CMC section
FDA’s guidance on formal meetings describes the general structure, but the substantive CMC expectations for a novel biologic include:
1. Drug substance description and characterization
- Molecular description — sequence, structure, modifications, mechanism of action
- Source materials — cell line origin and history, master and working cell banks
- For gene and cell therapies: vector design, transgene, packaging system, starting material qualification
- Identity, purity, potency, and safety characterization performed to date
- Critical quality attributes (CQAs) identified or under investigation
2. Manufacturing process overview
- Process flow diagram from starting material to drug substance
- Description of key unit operations — upstream (cell culture, transfection or fermentation), harvest, downstream (clarification, capture, polishing, formulation)
- Identification of critical process parameters (CPPs) — even if ranges are not yet defined, the parameters known to influence CQAs should be named
- In-process controls and hold times
- Manufacturing site(s) and a statement of GMP compliance status
- Scale of clinical manufacturing relative to development scale
3. Drug product description and formulation
- Composition, dosage form, container closure system
- Formulation development summary — buffer, excipients, concentration rationale
- Drug product manufacturing process overview
- Storage conditions and proposed shelf life
4. Analytical control strategy
- List of release tests for drug substance and drug product
- Methods used (with qualification status — qualified, validated, or under development)
- Proposed acceptance criteria, even if preliminary
- Reference standard strategy
- Potency assay strategy — for biologics, this is often a focal area for FDA
5. Stability program
- Stability data available to date (real-time and accelerated)
- Stability-indicating methods
- Proposed storage conditions and clinical use period
- Plan for ongoing stability through the clinical trial
6. Safety-relevant CMC considerations
- Adventitious agent testing strategy — particularly for biologics and cell/gene therapies
- Viral clearance considerations
- Endotoxin, sterility, mycoplasma, bioburden controls
- Impurity profile and toxicological qualification of significant impurities
Maturity expectations at pre-IND stage
A common source of sponsor anxiety: “We don’t have all of this yet — should we wait?” Usually no. FDA understands that pre-IND is, by definition, before final IND-enabling work is complete. What the agency wants to see is:
| CMC element | Expected maturity at pre-IND |
|---|---|
| Manufacturing process | Defined, with tox lot already produced or imminent; clinical lot manufacturing scheduled |
| Analytical methods | Qualified for release testing of tox material; validation in progress for clinical release |
| Reference standard | Identified and qualified, with bridging plan if it will change before clinical |
| Stability | 3-6 months of real-time data on representative material; accelerated underway |
| Specifications | Preliminary, with rationale; final specifications expected by IND |
| Process characterization | Initial; full characterization not expected until later phases |
| Comparability between lots | Demonstrated between tox and clinical material if they differ |
Gaps are acceptable; vague hand-waving is not. If a method is still under development, say so and describe the plan. If specifications are preliminary, say so and describe how they were set. FDA reviewers respect candor about development status. They penalize sponsors who appear to be hiding immaturity.
Framing the questions for FDA
The questions section is where the briefing package either creates value or wastes the meeting. Good pre-IND CMC questions share four characteristics:
- Specific. Not “Is our CMC plan adequate?” but “Does FDA agree that the proposed potency assay strategy described in Section 4.3 is acceptable to support Phase 1?”
- Decision-forcing. The question should require a yes/no/qualified position, not just a comment.
- Accompanied by your proposed position. State what you intend to do and your rationale. Ask FDA to confirm, comment, or object.
- Backed by adequate detail. The briefing package must contain enough information for FDA to evaluate the question. A question without supporting context will get a non-committal answer.
Common high-value CMC questions for novel biologics at pre-IND:
- Acceptability of the proposed potency assay strategy for first-in-human
- Acceptability of the proposed specifications, particularly for novel CQAs
- Comparability strategy if tox material and clinical material differ in process or scale
- Reference standard strategy and bridging plans
- Specific adventitious agent testing approach for novel cell lines or modalities
- Stability data package adequacy to support proposed clinical use period
- Acceptability of release testing strategy where assays are still in development
- Approach to characterization of product-related impurities or variants
The role of analytical methods in pre-IND strategy
Analytical methods are disproportionately important in CMC reviews of novel biologics because methods are how you demonstrate that what you put in the patient is what you intended to put in the patient. Key analytical attributes for IND filing typically include identity, content, potency, purity (size and charge variants for proteins; full:empty and aggregation for gene therapies), and safety attributes (sterility, endotoxin, mycoplasma, adventitious agents).
At pre-IND, FDA will evaluate whether your analytical control strategy is appropriate for the molecule and the proposed clinical use. Specific concerns the agency raises frequently:
- Potency assays that are not stability-indicating or not linked to mechanism of action
- Identity tests that are insufficiently specific (e.g., relying solely on SDS-PAGE for a complex biologic)
- Inadequate orthogonal methods for critical attributes
- Methods that cannot detect the relevant impurities for the modality
Understanding the distinction between analytical development versus process development matters here — both must mature in parallel, and an analytical program that lags the process leaves you unable to demonstrate process control.
Common deficiencies in pre-IND CMC packages
The most frequent issues that produce unhelpful FDA responses:
- Missing potency strategy. “Potency assay in development” without describing what the assay will measure, why it’s mechanism-relevant, or when it will be available.
- Reference standard ambiguity. No clear answer to what material is the reference standard and how it relates to tox and clinical material.
- Hand-waved stability. Stability “ongoing” without data, methods, conditions, or specifications.
- No discussion of comparability. When tox and clinical material differ — different scale, different facility, different process — comparability must be addressed proactively.
- Generic safety testing strategy. Boilerplate sterility/endotoxin/mycoplasma without addressing modality-specific risks (e.g., adventitious agents in a novel cell line, replication-competent virus testing for AAV).
- Specifications without justification. Numerical limits proposed without explanation of how they were derived.
- No CMC-specific questions. Sponsors who use the meeting only for clinical/nonclinical questions waste a free opportunity for CMC alignment.
Practical timeline for pre-IND CMC preparation
For a sponsor planning to file IND 6-9 months after pre-IND, a realistic CMC preparation timeline:
- 4 months before meeting: Internal scoping — what questions matter, what data will be available, what gaps need to be addressed before submission
- 3 months before meeting: Cross-functional CMC writing team assembled, briefing package outline locked, data cutoffs agreed
- 2 months before meeting: Draft sections complete, internal review, questions refined
- 60 days before meeting: Meeting request and briefing package submitted to FDA (per agency guidance)
- 30 days before meeting: Sponsor receives preliminary written responses from FDA; team prepares for any follow-up discussion
- Meeting day: Focused on areas where written responses were unclear or where dialogue adds value
- Post-meeting: Final meeting minutes from FDA become part of the regulatory record
FDA’s written responses, which arrive before the meeting, are often the most important deliverable. The meeting itself is for clarification, not for re-litigating the written positions.
Frequently asked questions
- How long should the CMC section of a pre-IND briefing package be?
- For a novel biologic, the CMC section is typically 30-60 pages of focused content, plus appendices. Excessively long packages frustrate reviewers; thin packages prevent informed answers. Aim for completeness in coverage and concision in writing.
- Can we ask FDA to comment on a CMC plan that’s not finalized?
- Yes, and you should. Pre-IND is specifically intended for this. Present your proposed plan, explain your rationale, and ask whether FDA has concerns. Wait until you have a “final” plan and you’ve waited too long.
- Should we submit the manufacturing process flow diagrams in the briefing package?
- Yes. Process flow diagrams are one of the most useful pieces of information for a CMC reviewer to orient quickly. Include them with key process parameters annotated.
- Do we need GMP material to hold a pre-IND meeting?
- No. Pre-IND can occur before GMP clinical manufacturing has begun. You should, however, be able to describe the GMP manufacturing plan, site, and timeline.
- What’s the biggest predictor of a useful pre-IND CMC outcome?
- Quality of the questions. Sponsors who ask specific, position-stated, decision-forcing questions get specific, useful answers. Sponsors who ask open-ended questions get cautious, non-committal answers. Invest in the questions list — it determines the value of the entire meeting.
Closing thoughts
A pre-IND meeting is one of the few opportunities to align with FDA on CMC strategy before formal review begins. For novel biologics, where regulatory pathways are less well-trodden, this alignment is genuinely de-risking — both for your IND submission and for the broader development plan. The CMC content in the briefing package should be specific, candid about maturity, and structured around questions where FDA’s input will change what you do next.
DES Pharma Consulting supports sponsors in scoping and preparing pre-IND briefing packages, with particular focus on CMC strategy for novel biologics, gene therapies, and cell therapies. If you’re approaching your pre-IND meeting, the time to start scoping the CMC content is now.

Matt specializes in Process Development (PD) and Chemistry, Manufacturing, and Controls (CMC) strategy, helping life sciences companies navigate early-stage development, lab innovation, and technical regulatory hurdles.
Reach out to Matt on LinkedIn.



